
Routine Intervention in Labour
Routine Intervention in Labour
Every woman wants to have the best possible care during the birth of her baby. She wants to feel that her needs and the needs of her baby, are placed front and centre in all decisions. Athough this is the ideal situation, there may a tension between meeting the individual needs of women and the routines and policies of the hospital the they have chosen to look after them.
Routine interventions are generally seen as necessary in order to keep the mother and baby safe during the birth. Some interventions may have negative impacts or side effects. They might:
- interfere with the physiology of the labour process;
- separate the woman from her partner, other support people, baby, or caregivers;
- be uncomfortable and unpleasant;
- have other more serious side-effects
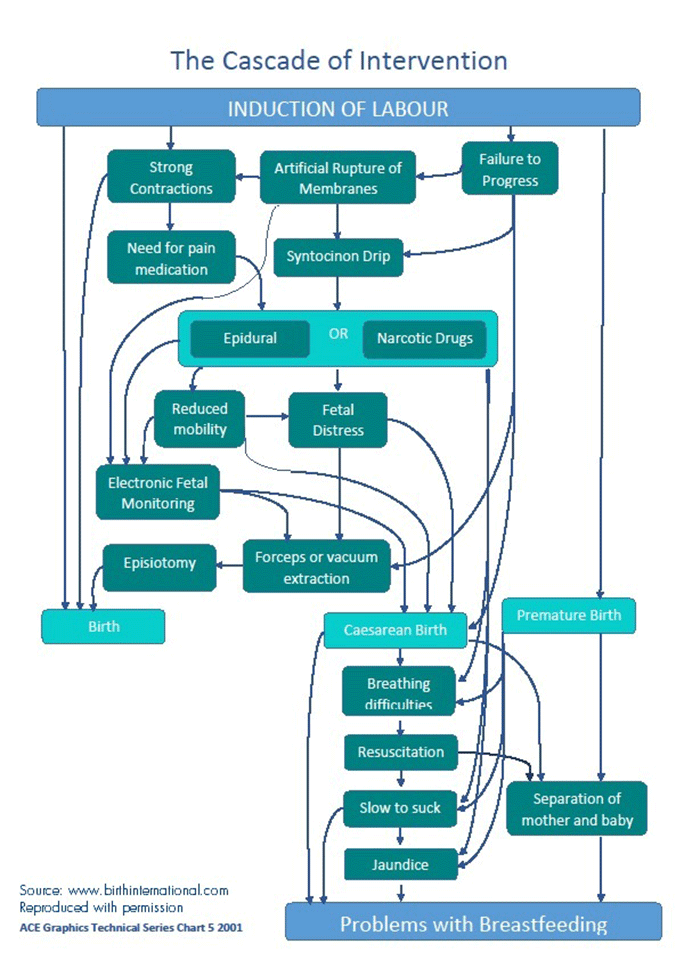
- lead to the use of other interventions designed to monitor, prevent or treat these side effects (known as the Cascade of Intervention).
We might see these negative impacts as necessary trade offs if they mean that labour and birth are safer for our babies. However, there is now growing evidence that some of these routine procedures as well as potentially interfering or causing harm, do not actually benefit the woman or baby.
Which routine interventions cause harms but have no benefit to either mother or baby?
Research shows that the following forms of care or procedures increase risks and have no benefit to the mother and baby:
Recording a woman's progress in labour using a Partogram (Lavender et al. 2013 link).
A Partogram is a graph of a woman's progress in labour made by the midwife by using results from Abdominal Palpation and Vaginal examinations.
- increased the risk of being diagnosed with a prolonged labour and experiencing further intervention to address the diagnosis (Albers 1999, Cesario 2004 and Zhang et al. 2002, Walsh 2009, Walsh 2012, Lavender et al. 2013)
Offering vaginal examinations during labour (Downe et al.2013 link).
- increases emotional distress (NICE 2007, Devane. 1996, Lewin et al. 2005).
- increases the risk of infection to the baby (Lumbiganon et al. 2004, Seaward et al. 1997 and Hannah et al. 2000).
Monitoring the baby's heart rate with the doppler in low risk women (Alfirevic et al. 2010 link).
- routine doppler ultrasound is not recommended in low-risk pregnancies (NICE 2007:35)
Continuous electronic fetal monitoring – the belt monitors (Alfirevic et al. 2013 link).
- More likely to have minor obstetric interventions like epidural analgesia, ongoing continuous electronic fetal monitoring and fetal blood sampling for fetal distress (Blix 2005);
- Increases the risk of a vacuum or forceps assisted birth (Alfirevic et al. 2013);
- increases the risk of having a caesarean (Alfirevic et al. 2013);
Artificially breaking the waters (Smyth et al. 2013 link).
Lying down during labour or birth (Lawrence et al. 2013 link).
- increases the duration of labour (Lawrence et al.2013).
- increases the risk of caesarean birth (Lawrence et al.2013).
- increases the need for epidural (Lawrence et al.2013).
- increases risk of significant bleeding (Terry et al. 2006)
- increases risk of anal sphincter tear (Dudding et al. 2008)
Coach pushing for the birth when the woman does not have an epidural in place (Bloom et al. 2006 link)
- Increases the risk of pelviic floor damage (Fraser et al. 2000, Schaffer et al.2005, Handa et al.1996).
Cutting an episiotomy for any reason other than the baby being distressed (Dannecker et al. 2004 link)
- increases the risk of significant pelvic floor damage (Carroli and Mignini 2009, DiPiazza et al. 2006, Gerdin et al. 2007, Altman et al.2007, Sartore et al.2004, Bick et al. 2008, Dannecker et al. 2004).
Giving low risk women an injection of artificial oxytocin to deliver the placenta (Begley at al.2011 link)
- increases blood pressure;
- increases after pains;
- increases the risk of nausea and vomiting;
- increases the use of medication for pain relief in the postnatal period;
- increases the number of women readmitted to hospital with vaginal bleeding (Begley at al. 2011).
PPA campaigns to support maternity services to ensure that their clinical guidelines reflect the best evidence available and that midwives and doctors present this information to women so that they can make informed decisions about their care. If you would like to get involved as a maternity consumer, you will find further details here.
References
- Albers, L. (1999) the duration of labour in healthy women. Journal of Perinatology. 19(2): 114-19.
- Alfirevic, Z., Devane, D., Gyte, G.M.L. (2013), Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. Editorial Group: Cochrane Pregnancy and Childbirth Group. Published Online: 31 MAY 2013 available at http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD006066.pub2/abstract [accessed on 15 November 2013].
- Altman, D., Ragnar, I. and Ekstrom, A. (2007). Anal sphincter lacerations and upright delivery postures: a risk analysis from a randomized controlled trial. International Urogynecology Journal, 18: 141-6.
- Begley CM, Gyte GML, Murphy DJ, et al. (2011) Active versus expectant management for women in the third stage of labour. Cochrane Database of Systematic Reviews, Issue 11. Chichester: John Wiley and Sons
- Bick, D., MacArthur, C. and Winter. H. (2008) Postnatal Care: Evidence and Guidelines for Management, 2nd edn. London: Churchill Livingstone.
- Blix, E., Reinar, L. and Klovning, A. and Oian, P. (2008) Prognostic value of the admission test and its effectiveness compared with auscultation only: a systematic review. BJOG, 112: 1595-604.
- Caldeyro-Barcia, R. (1979) Influence of maternal bearing down efforts during second stage on fetal well-being. Birth and Family Journal, 6(1): 7-13.
- Carroli, G. and Mignini, L. (2009) Episiotomy for vaginal birth. (Cochrane Review). In The Cochrane Library, Issue 1. Chichester: John Wiley & Sons, Ltd.
- Cesario, S. (2004) Re-evaluation of Freidman’s labour curve: a pilot study. Journal of Obstetrics, Gynecology and Neonatal Nursing, 33:713-22.
- Dannecker, C., Hillemanns, P. Strauss, A. et al. (2004) Episiotomy and perineal tears presumed to be imminent: randomised controlled trial. Acta Obstetrics et Gynecologica Scandinavia, 83: 364-8.
- Devane, D. (1996) Sexuality and Midwifery. British Journal of Midwifery, 4(8): 413-20.
- DiPiazza, D., Richter, H., Chapman, V., Cliver, S., Neely, C., Chen, C. and Burgio, K. (2006) Risk factors for anal sphincter tear in multiparas. Obstetrics and Gynecology, 107(6): 1233-6.
- Downe S, Gyte GM, Dahlen HG, Singata M. (2013). Routine vaginal examinations for assessing progress of labour to improve outcomes for women and babies at term. Cochrane Database Syst Rev. 2013 Jul 15;7:CD010088. doi: 10.1002/14651858.CD010088.pub2.
- Fraser, W., Marcoux, S., Krauss, I. et al. (2000) Multi-centre, randomised controlled trial of delayed pushing for nulliparous women in the second stage of labour with continuous epidural analgesia. American Journal of Obstetrics and Gynecology, 182: 1165-72.
- Gerdin E, Sverrisdottir G, et al. (2007). The role of maternal age and episiotomy in the risk of anal sphincter tears during childbirth. Aust N Z J Obstet Gynaecol 47 (4): 286-90.
- Handa, V., Harris, T. and Ostergard, D. (1996) Protecting the pelvic floor: obstetric management to prevent incontinence and pelvic organ collapse. Obstetric and Gynecology, 88: 470-8.
- Hannah M.E., Hannah, W.I., Hewson, S.A., et al. (2000) Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Lancet 2000; 256: 1375-83.
- Hodnett ED, Downe S, Walsh D. (2012). Alternative versus conventional institutional settings for birth. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD000012. DOI: 10.1002/14651858.CD000012.pub4.
- Johnstone, F., Aboelmagd, M. and Harouny, A. (1987) Maternal position in the second stage of labour and fetal acid base status. British Journal of Obstetrics and Gynaecology, 94(8): 753-7.
- Lavender, T., Hart, A., Smyth, R. (2013). Effect of partogram use on outcomes for women in spontaneous labour at term. Editorial Group: Cochrane Pregnancy and Childbirth Group. Published Online: 10 JUL 2013 at :http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005461.pub4/abstract . DOI:10.1002/14651858.CD005461.pub4
- Lawrence, A., Lewis, L., Hofmeyr, G.J., Styles, C. (2013). Maternal positions and mobility during first stage labour. Editorial Group:Cochrane Pregnancy and Childbirth Group. Available online at http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003934.pub4/abstract [Accessed on 1 April 2014]
- Lewin, D., Fearon, B., Hemmings, V., & Johnson, G. (2005). Women's experiences of vaginal examination in labour. Midwifery, 21, 267-277.
- Lumbiganon, P., Thinkhamrop, J., Thinkhamrop, B., & Tolosa, J. E. (2004). Vaginal chlorhexidine during labour for preventing maternal and neonatal infections (excluding Group B Streptococcal and HIV). Cochrane Database of Systematic Reviews (4). The Cochrane Collaboration retrieved 17/04/09.
- NICE (2007) Intrapartum care: Care of healthy women and their babies during childbirth. Available online at http://www.nice.org.uk/nicemedia/pdf/IPCNICEguidance.pdf [accessed on 6 September 2013]
- Sandall, J., Soltani, H., Gates, S. et al (2013). Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database of Systematic Reviews, Issue 8. Available online at http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004667.pub3/abstract [accessed on 31 October 2013].
- Sartore, A., De Seta, F., Maso, G. et al. (2004) The effects of mediolateral episiotomy on pelvic floor function after vaginal delivery. Obstetrics and Gynecology, 103: 669-73.
- Schaffer, J., Bloom, S., Casey, B. et al. (2005) A randomised trial of the effect of coached vs uncoached maternal pushing during the second stage of labor on postpartum pelvic floor structure and function. American Journal of Obstetrics and Gynecology, 192: 1692-6.
- Seaward PG, Hannah ME, Myhr TL, et al. International Multicentre Term Prelabor Rupture of Membranes Study: evaluation of predictors of clinical chorioamnionitis and postpartum fever in patients with prelabor rupture of membranes at term. American Journal of Obstetrics and Gynecology. 1997;177(5):1024–9.
- Smyth, M.D., Markham, C., Dowswell, T. (2013). Amniotomy for shortening spontaneous labour. Editorial Group: Cochrane Pregnancy and Childbirth Group. Published Online: 18 JUN 2013, available at http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD006167.pub4/abstract [accessed on 15 November 2013]. DOI: 10.1002/14651858.CD006167.pub4.
- Walsh, Denis (2012) Evidence and Skills for Normal Labour and Birth – A Guide for Midwives. Second Edition. New York: Routledge.
- Walsh, T. (2009) Exploring the effects of hospital admission on contraction patterns and labour outcomes using women’s perception of events. Midwifery, 25: 242-52.
- Zhang, J., Troendle, J. and Yancey, M. (2002) Reassessing the labour curve. American Journal of Obstetrics and Gynecology, 187: 824-8.
QUICK FACTS
The following interventions cause harms without benefits:
Vaginal Examinations
It does not benefit the woman or baby to know how dilated the cervix is during labour.
Belt Monitors
It does not benefit the woman or baby of any risk status, to have external Continuous Electronic Fetal Monitoring or CTG during labour
Breaking the waters
It does not benefit the woman or the baby to routinely have the membranes artificially ruptured during labour.
Episiotomy
It does not benefit the woman to have an episiotomy. The only benefit is to a distressed baby.